We have known about the failure for decades. What has changed is not the diagnosis. It is that we have run out of room to manage around it.
For a long time, the fragmentation in our care system was visible, documented, and largely tolerated. It was built into the structure. Incentives rewarded episodes rather than continuity, which meant the system organized itself around discrete events, a hospitalization, a procedure, a discharge, rather than around the arc of a person’s life. We created institutions, programs, and categories to support those events, and over time, we began to call that a system, even though it rarely behaved like one.

AgeTech emerged as a serious attempt to address parts of this. It brought real progress. We have better connectivity, more data, and a level of integration that did not exist before. That infrastructure matters. It is a necessary foundation.
But infrastructure, on its own, does not solve the problem. And a decade in, it is worth asking whether the way we framed the problem has started to limit how we approach it.
Age is a convenient organizing principle. It is also a blunt one. It tells you very little about what someone actually needs. A 70-year-old launching a company and a 70-year-old managing multiple chronic conditions in a rural community are not facing the same problem. A parent coordinating care for a child with complex needs is encountering many of the same system failures, just at a different point in life. These are not separate markets. They are different people running into the same structural limits from different directions.
What we have been trying to solve was never about age. It is what happens when life becomes more complex than the system can coherently manage, and when the responsibility for holding that complexity together quietly shifts to individuals and families who were never meant to carry it alone. That dynamic shows up most clearly in the parts of the system under the greatest strain, in rural settings, in lower-resourced communities, in IDD, but it is not unique to them. It is the same structural issue, more visibly exposed.
You see it most clearly in transitions. When someone moves from one setting to another, particularly from institutional care back into the community, nothing formally breaks. The discharge happens. The follow-ups are scheduled. The plan exists on paper.
But something essential is lost.
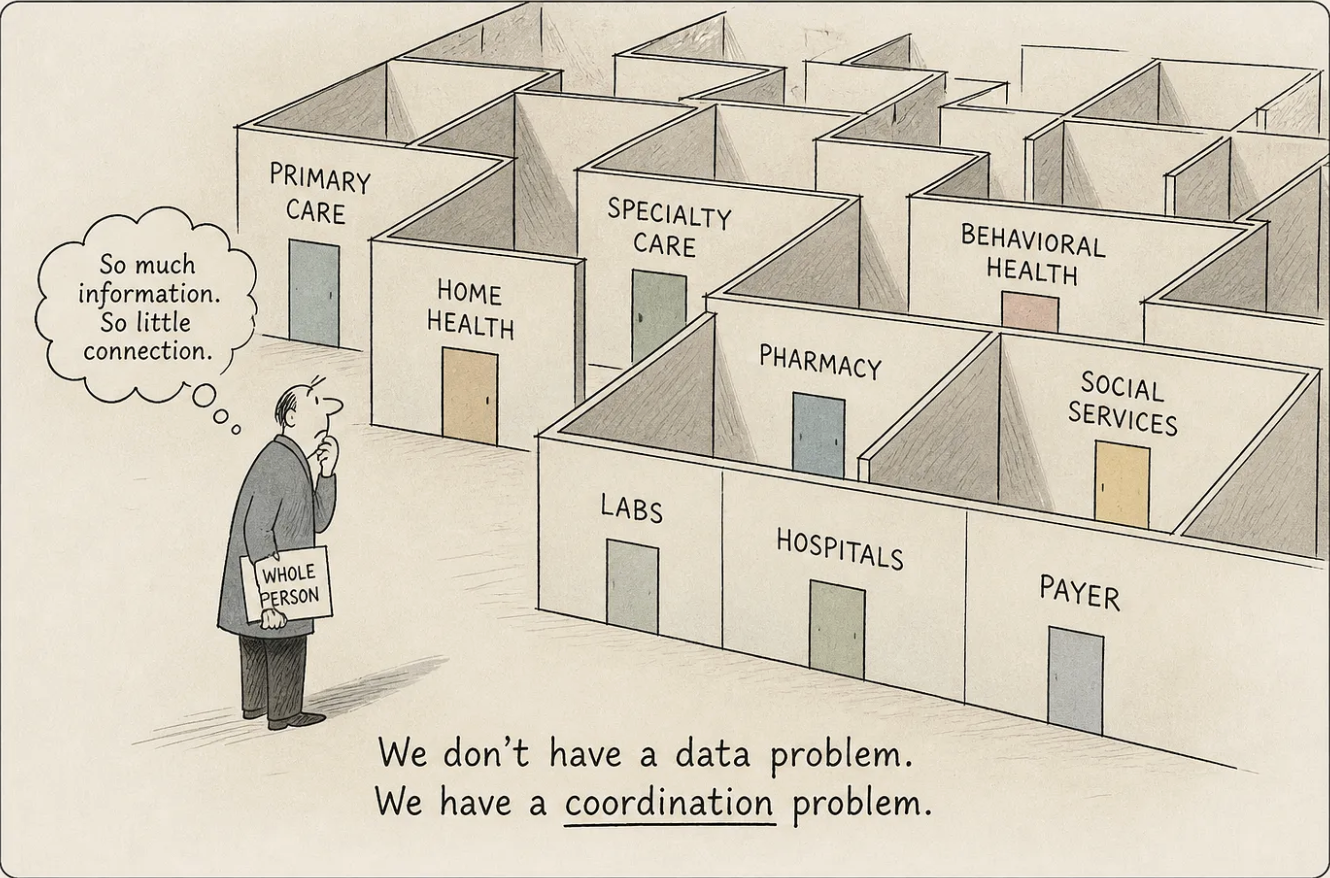
Responsibility is shared among providers, families, and community-based organizations, each with partial visibility. At the same time, more information than ever is being generated: devices, platforms, and records, each capturing a piece of what is happening.
In the days that follow, the signals begin to appear. A missed medication. A family member’s comment that something feels off. A direct support professional notices a shift that does not quite meet a reporting threshold. None of these requires action on its own.
That is precisely the problem.
They do not come together. They remain scattered across people, systems, and time. No one is responsible for holding them long enough to see what they might mean when viewed together. By the time something is clear enough to demand action, the earlier opportunity has already passed.
The industry’s response to fragmentation was to connect more things. The logic was sound. If the problem is that information isn't shared, then sharing more should improve coordination.
For those building systems and for analysts working behind the scenes, more data can be useful. It reveals patterns, supports models, and improves understanding over time. But that is not where decisions are made.

On the front lines, where clinicians, direct support professionals, and families are making real-time decisions, more data often translates into more interpretation. More alerts. More dashboards. More signals that arrive without context. The question is rarely whether information exists. It is whether anyone can do something with it in the moment it matters.
The gap that matters is not between what is collected and what is missing. It is between what exists and what anyone can act on.
Coordination has followed a similar path. It has been treated as something we can ask people to do, rather than something the system is built to support. We created care teams, transition programs, and communication tools, but left the underlying incentives largely unchanged. Most providers are still paid on an episodic basis. Organizations still operate within their own boundaries. Families are still expected to bridge gaps that no individual should be responsible for bridging.
When coordination happens, it happens because someone made an extra effort. That is not a system. That is a workaround.
For a long time, we were able to absorb that. We tolerated inefficiency. We relied on informal caregiving. We accepted that some failures were simply part of the complexity.
What has changed is not the nature of the problem. It is the arithmetic.
The demographic shift has been visible for decades, but it now arrives in a way that removes the option of managing around the gaps. The number of older adults is growing faster than the system can absorb. The population of people living with disabilities is growing. The workforce available to support them is not keeping pace; in many settings, it is shrinking. The family infrastructure that has quietly carried an enormous share of the burden is under strain in ways that are only beginning to show. And public budgets are constrained in ways that make adding more funding to an inefficient structure not just difficult, but unrealistic.
The system can continue to add complexity. It cannot continue to absorb it.
The direction can no longer remain implicit. The question is not how to incrementally improve what exists. It is what the system actually needs to become, and how to move toward that while still operating inside today’s constraints.
That is a more difficult question than the ones we have been asking. It also leads to a more uncomfortable realization.
If the system continues to evolve along the same lines, more data, more tools, more attempts to coordinate within the same structure, it will become more complex without becoming more effective.

And complexity is exactly what it can no longer absorb.
Part Two takes up the harder question: not what went wrong, but what we are actually building toward.
Need a hand? Not sure where to start?
We're here and happy to help. Drop us a line and we'll get back to you or call Support at (877) 694-4431.
We also have tons of articles and videos on our help page for many frequently asked questions.
Privacy is important to us, so you have the option of disabling certain types of storage that may not be necessary for the basic functioning of the website. Blocking categories may impact your experience on the website. More information

